

Posterior Vitreous Detachment
Posterior Vitreous Detachment (PVD) is a natural change that occurs during adulthood, when the vitreous gel that fills the eye separates from the retina, the light-sensing nerve layer at the back of the eye.
Symptoms
- Floaters (mobile blurry shadows that obscure the vision)
- Flashes (streaks of light, usually at the side of the vision)
These symptoms usually become less intense over several weeks. Most patients experience PVD after age 60, once in each eye, and the condition is usually non-sight-threatening but occasionally affects vision more permanently in the event of complication, such as retinal detachment or epiretinal membrane.

Symptoms in detail
Mild floaters in the vision are normal, but a sudden increase in floaters is often the first symptom of PVD.
During PVD, floaters are often accompanied by flashes, which are most noticeable in dark surroundings. Most patients experience floaters and flashes during the first few weeks of a PVD, but in some cases the symptoms are hardly noticeable. If PVD is complicated by vitreous hemorrhage, retinal detachment, epiretinal membrane, or macular hole, the flashes and floaters may be accompanied by decreased or distorted vision. Floaters are most bothersome when near the center of vision and less annoying when they settle to the side of the vision. They may appear like cobwebs, dust, or a swarm of insects—or in the shape of a circle or oval, called a Weiss ring.
Causes
Over time, the vitreous gel that fills the eye becomes liquid and condenses (shrinks) due to age and normal wear and tear. Eventually it cannot fill the whole volume of the eye’s vitreous cavity (which remains the same size during adulthood) and so the gel separates from the retina, located at the very back of the eye cavity.

Figure 1. Diagram of the vitreous cavity during posterior vitreous detachment.
Over the next 1 to 3 months, the vitreous gel further condenses and the sides of the gel also separate from the retina until the PVD is complete and the vitreous gel is attached to the retina only at the vitreous base (see Figure 1). Clear vitreous fluid fills the space between the condensed vitreous gel and the retina.
If a PVD progresses gently, gradually, and uniformly, the symptoms are typically mild. However, if the forces of separation are strong or concentrated in a particular part of the retina, or if there is an abnormal adhesion (sticking together) between the vitreous gel and the retina (such as lattice degeneration), the PVD can tear the retina or a retinal blood vessel.
Flashes and floaters are typically more obvious when PVD is complicated by a retinal tear or vitreous hemorrhage. These conditions can lead to further complications, such as retinal detachment or epiretinal membrane, which can result in permanent vision loss. However, about 85% of patients who expe- rience PVD never develop complications and in most cases, the flashes and floaters subside within 3 months.
Risk factors
Posterior vitreous detachment is rare in people under the age of 40, and increasingly common during advanced age.
Additional risk factors for PVD include myopia (nearsighted- ness), trauma, and recent eye surgery such as a cataract operation. Patients who experience PVD in one eye will often experience PVD in the other eye within 1 year.
Diagnostic testing
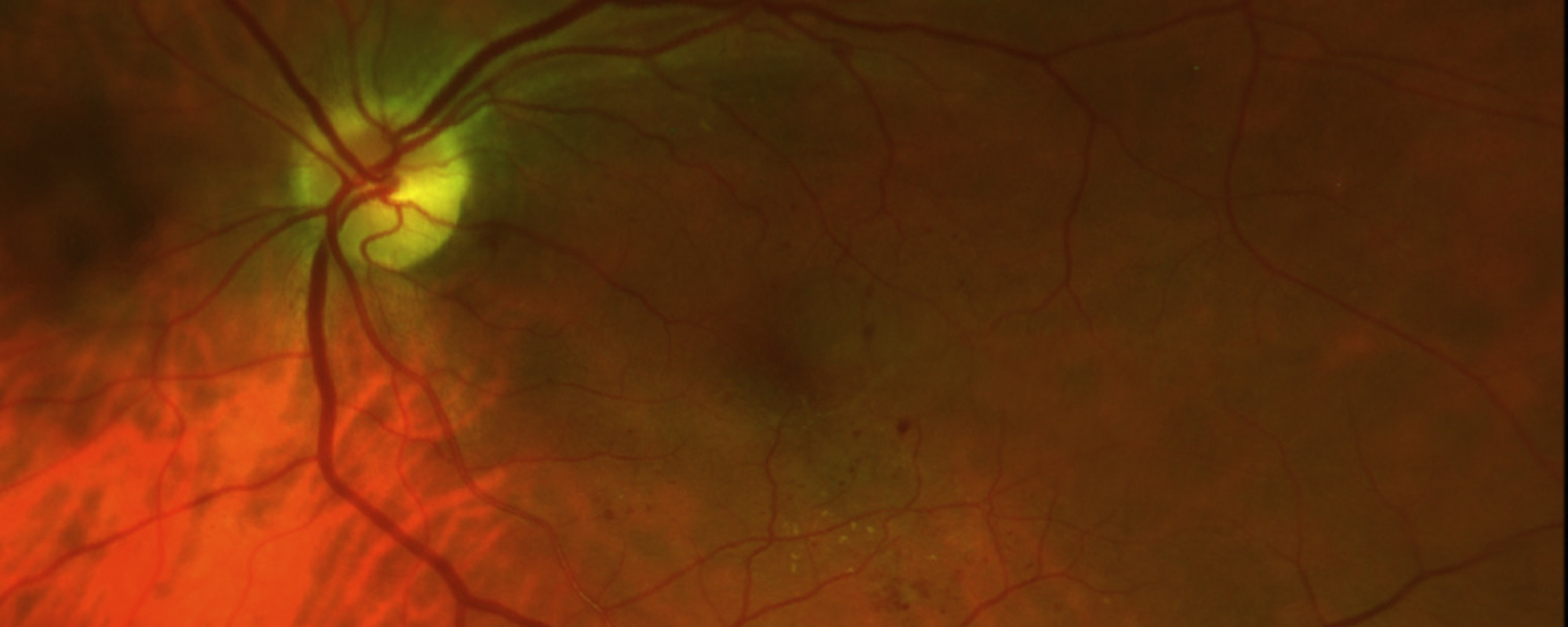
 Posterior vitreous detachment is usually diagnosed with a dilated eye examination. However, if the vitreous gel is very clear, it may be hard to see the PVD without additional testing, such as optical coherence tomography (OCT) or ocular ultrasound (see Figure 2).
Posterior vitreous detachment is usually diagnosed with a dilated eye examination. However, if the vitreous gel is very clear, it may be hard to see the PVD without additional testing, such as optical coherence tomography (OCT) or ocular ultrasound (see Figure 2).
Figure 2. Most posterior vitreous detachments can be diagnosed with a dilated eye exam. However, OCT (A) and B-scan ultrasound (B) are diagnostic tests that can be helpful in diagnosing PVD.
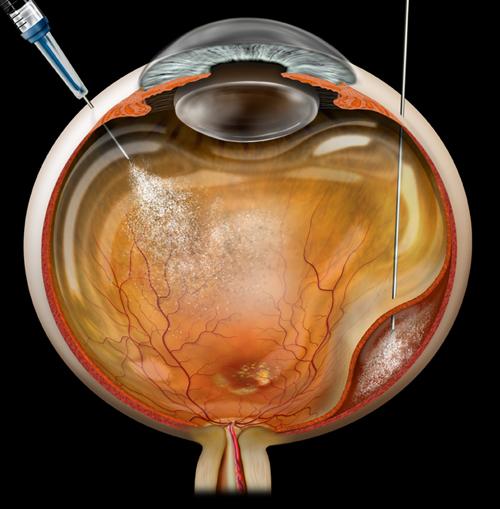
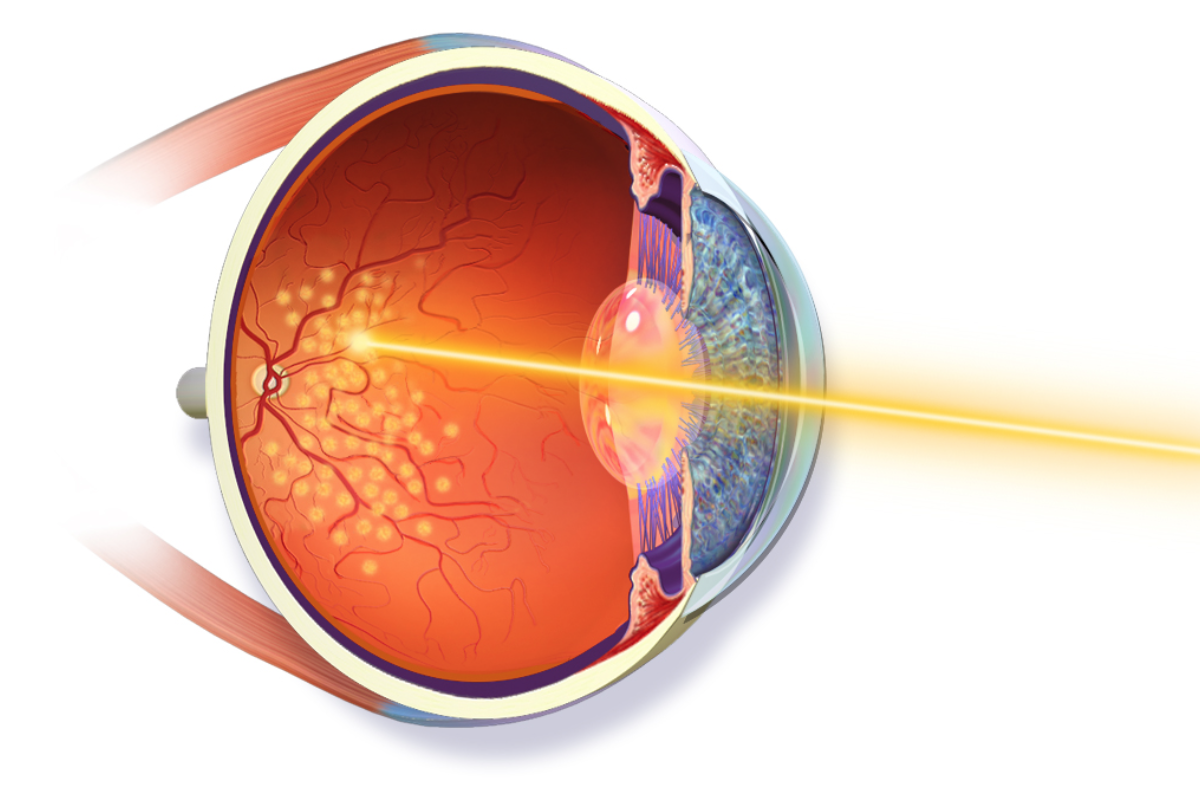
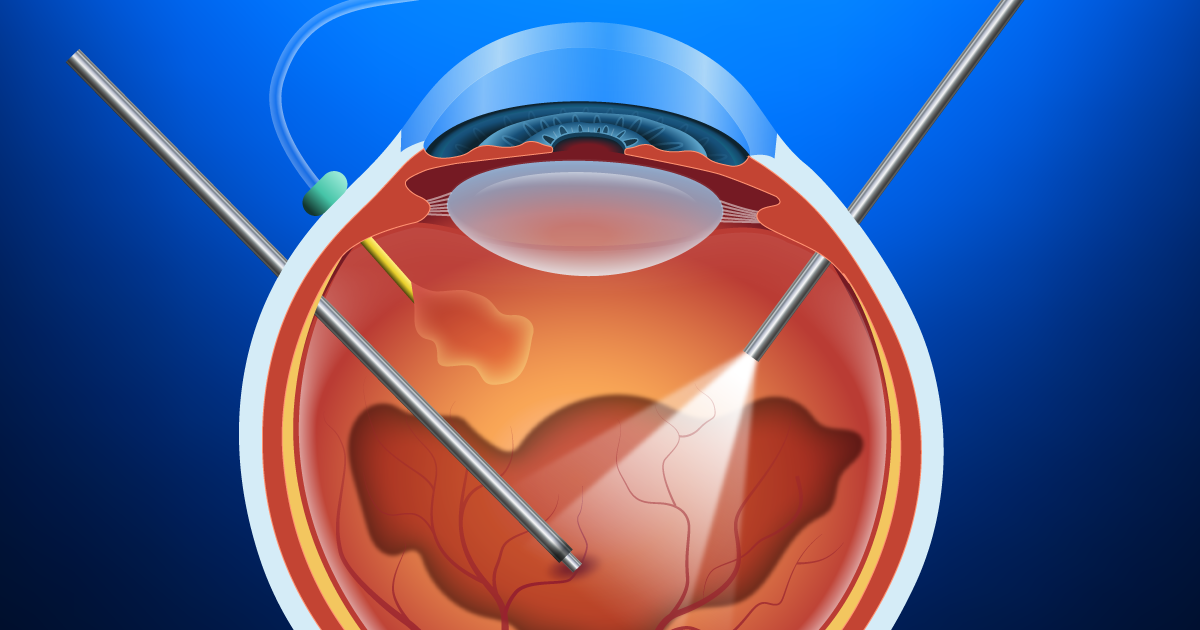
Treatment and prognosis
PVD is non-sight-threatening and the symptoms subside in the vast majority of patients. Most patients no longer notice flashes or floaters 3 months later, and no treatment or further check- ups are needed at that time. Complications of PVD are rare but can be serious and require urgent treatment, such as laser for a retinal tear or surgery for a retinal detachment. For this reason, one or more checkups are recommended within 3 months after the onset of PVD. Rarely, the floaters from PVD persist, and vitrectomy surgery to remove the floaters is effective; you and your doctor may consider this after discussing the risks and benefits of surgery.

