
What is a Scleral Buckle?
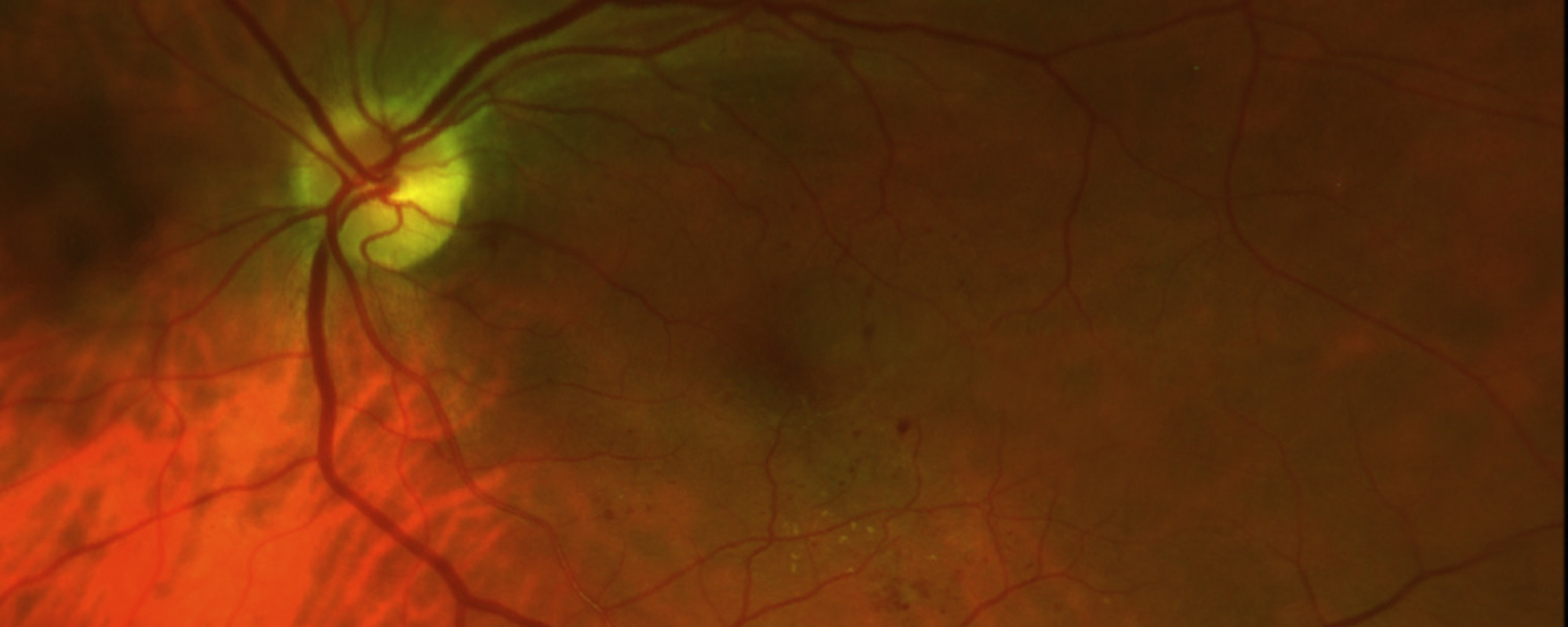
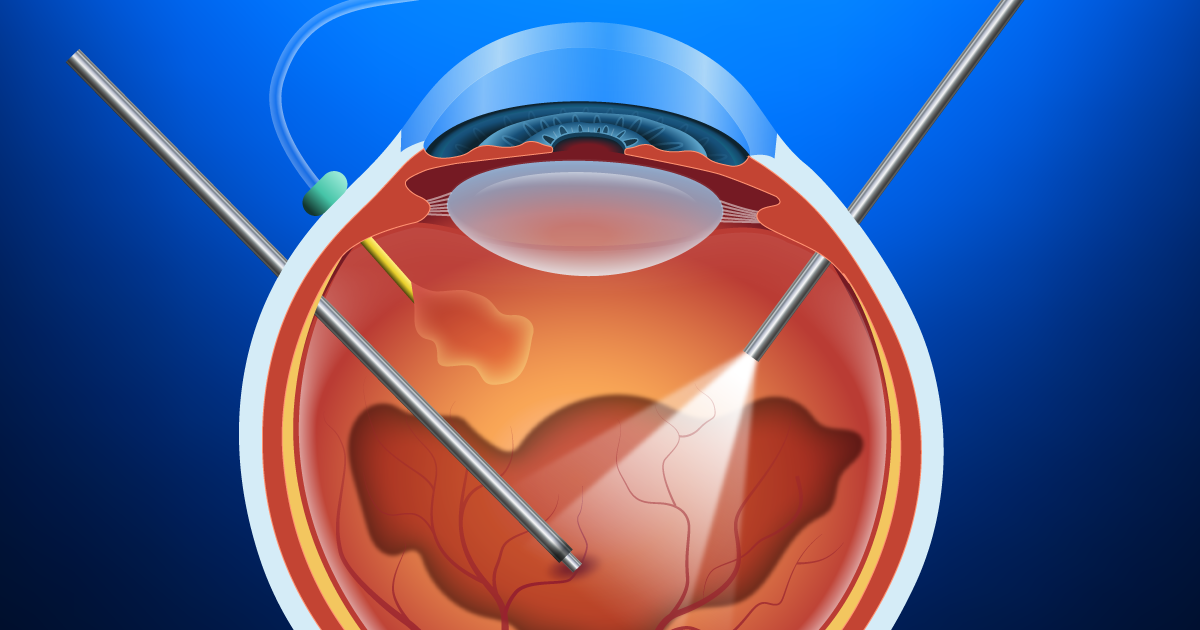
Scleral buckling surgery is a way to treat retinal detachment. Retinal detachment occurs when the two layers of the retina, the sensory retina and the retinal pigment epithelium (RPE), become separated from each other and from the wall of the eye. Retinal detachment can lead to severe vision loss or blindness.
A scleral buckle is a piece of silicone sponge, rubber, or semi-hard plastic that your eye surgeon places on the outside of the eye (the sclera, or the white of the eye). The material is stitched down to the eye to keep it in place. The buckling element is usually left in place permanently. The element pushes in, or “buckles,” the sclera toward the middle of the eye. This buckling effect on the sclera relieves the pull (traction) on the retina, allowing the retinal tear to settle against the wall of the eye. The buckle effect may cover only the area behind the detachment, or it may encircle the eyeball like a ring
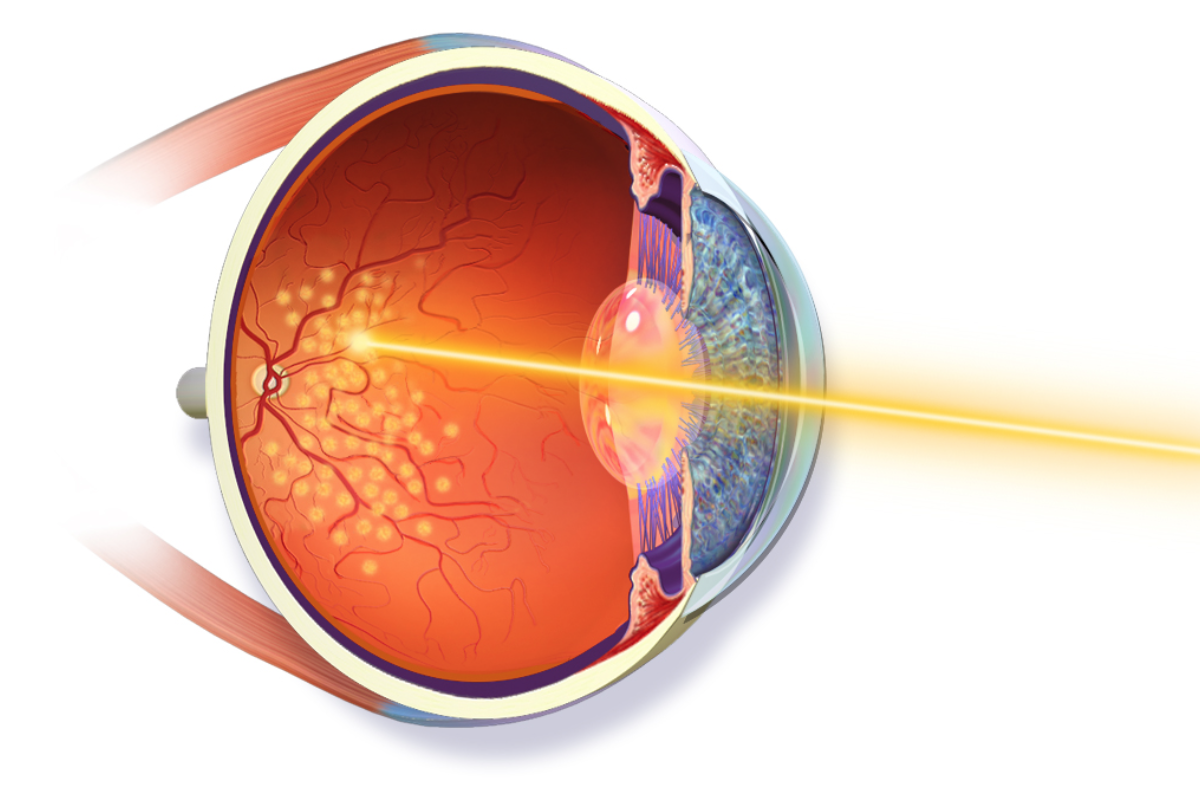
Usually extreme cold (cryopexy) or heat (diathermy) or light (laser photocoagulation) is used to treat the retina and hold it in place until a seal forms between the retina and the layer beneath it. The seal holds the layers of the eye together and keeps fluid from getting between them.
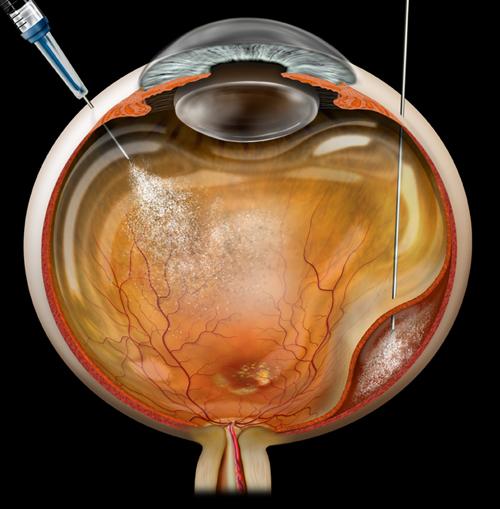
Your ophthalmologist may inject a gas bubble into your eye to flatten the retina. He or she may also drain the fluid under the detached retina through a tiny hole in the sclera. If there is only a small amount of fluid, draining it may not be needed. The retina can remove small amounts of fluid by itself.
What are the risks?
Scleral buckling poses some short-term and long- term risks.
Detachment of the choroid, the middle layer of tissue that forms the eyeball, is a common complication of scleral buckling surgery. Choroidal detachments usually heal on their own within about 2 weeks without further treatment. The pressure of the scleral buckle can raise the fluid pressure inside the eyeball. People with glaucoma may have a higher risk of this complication.
The eye may become infected. You may need antibiotics and corticosteroids to reduce redness or discharge from the eye and treat the infection. Sometimes it is necessary to remove the buckling implant to treat the infection.
You may have swelling or inflammation of the macula (the central portion of the retina), other parts of the retina, or the membranes surrounding the retina.
The silicone plastic or rubber of the buckling device may rub on other parts of the eye, move out of place, or become a site of infection. In some cases, the buckling device may need to be removed.
A scleral buckle can change the shape of the eye, changing your refraction (power of your glasses). You may need glasses or contact lenses (or a new prescription) to correct the changes.
The scleral buckle can affect the eye muscles and how well they control the movement of the eyes. This can lead to misaligned eyes (strabismus) and double vision (diplopia).
The scleral buckle can affect the eyelids and cause ptosis or droopy eyelid.
What can I expect after the surgery?
Placing a scleral buckle reattaches the retina in most cases.
Chances for good vision after surgery are higher if the macula was still attached before surgery. If the detachment affected the macula, good vision after surgery is still possible but less likely.
What type of anesthesia is used?
Scleral buckle surgery is performed under local (injection) or anesthesia, with sedation. General anesthesia may be used instead in some cases. Retinal detachment surgery is usually performed as an outpatient (day surgery) procedure. In some cases a hospital stay overnight may be required.

